
Ephedra sinica
By Joshua Miller, PhD
Published in the December 2024 issue of Clinical & Forensic Toxicology News
The plant species of the Ephedra genus are gymnosperm shrubs that have been used in herbal medicine for millennia to treat allergies, asthma, colds, fever, etc., due to their naturally occurring ephedrine alkaloids (ephedra) (1). These plants can be found in arid regions of Asia, Europe, Northern Africa, North America, and South America. Ephedra has been used in traditional Chinese medicine for more than 5,000 years where the crude extract of the aerial parts of either E. sinica, E. equisetina, or E. intermedia is known as Ma Huang (“yellow hemp”; Fig. 1). Of these species, E. sinica (Chinese ephedra) is the most widely used and is native to arid regions of Mongolia, Russia, and China, where it grows on hillsides, plains, dry wastelands, riverbeds, and grasslands (2). The desired alkaloids from Ma Huang are traditionally extracted by boiling dried stems in water and preparing a hot tea (1, 3). The association of preparing tea from Ephedra is noted in the common names of several Ephedra species, such as “Mormon tea” (E. californica and E. nevadensis), “Desert tea” (E. californica), or “Mexican tea” (E. torreyana), although North American Ephedra do not contain ephedrine alkaloids (4).

Figure 1. Ephedra sinica (Chinese ephedra) at the Berlin Botanic Garden and Botanical Museum. Reproduced with permission from Krzysztof Ziarnek, Kenraiz/Wikimedia Commons/CC-BY-SA-4.0
In more recent history, E. sinica has found use in herbal supplements where it was often combined with caffeine to support weight loss and boost energy. Because dietary supplement ingredients in use before October 15, 1994, do not require additional safety data before marketing, it was once possible to purchase supplements containing ephedra in the United States. However, as early as 1997, the United States Food and Drug Administration (FDA) began proposing new rules on the allowable amount of ephedrine alkaloids sold in supplements, although these rules were withdrawn in 2000. Ultimately, the FDA issued a final regulation, effective April 12, 2004, which prohibited the sale of supplements containing ephedra (5).
The most abundant ephedrine alkaloids of Eurasiatic Ephedra are (1R,2S)-ephedrine and (1S,2S)-pseudoephedrine, which are diastereomers of one another and precursors in methamphetamine production, Fig. 2 (4).
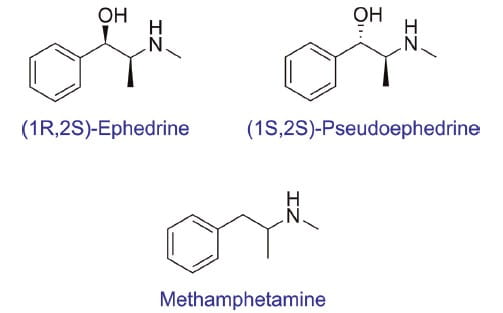
Figure 2. Structures of abundant ephedrine alkaloids present in Eurasiatic Ephedra (top), which are structurally like methamphetamine (bottom).
Ephedrine is both a direct and indirect sympathomimetic amine. It is an agonist of α- and β-adrenergic receptors but also prevents neuronal norepinephrine uptake, which enhances norepinephrine’s own α- and β-adrenergic action. Thus, ephedrine stimulates a sympathetic response in the user that increases heart rate, raises blood pressure, dilates the bronchi, and diverts blood flow to skeletal muscles (6). Pseudoephedrine is also an indirect sympathomimetic amine but only has a-adrenergic action and stimulates a weaker sympathetic response compared to ephedrine (7).
The naturally occurring content of ephedrine alkaloids in Ma Huang varies, but tea prepared from Ma Huang has 10–30 mg of ephedrine per serving depending on brewing methods. Before their ban, herbal supplements contained a range of 1.1–15.3 mg of ephedrine per dosage unit (8, 9). Clinically, ephedrine is administered intravenously as either a hydrochloride or sulfate salt, with starting doses of approximately 5 mg to a maximum dosage of approximately 50 mg. Pseudoephedrine is administered orally as a hydrochloride salt with a starting dose of 60 mg to a maximum of 240 mg every 24 hours (10–12). After consumption, both drugs can engender a response in as little as 15 minutes, with peak concentrations occurring at 1.5 to 2.4 hours for pseudoephedrine and 1.28 to 3.90 hours for ephedrine post-consumption (11, 13, 14). Both ephedrine and pseudoephedrine are mostly excreted unchanged in urine, with a half-life of 6 hours and 4–6 hours, respectively. However, given that both drugs are bases, their elimination is prolonged in alkaline urine due to decreased solubility (15).
Because ephedrine and pseudoephedrine have adrenergic action, Ma Huang has been used for thousands of years to treat asthma. Today, ephedrine is still used for allergy relief due to its bronchodilatory effects. Ephedrine is also clinically indicated to treat hypotension perioperatively. It is commonly used to counteract hypotension in the setting of spinal anesthesia and is sometimes preferred over other vasopressors because it maintains uterine blood flow (6). Because pseudoephedrine is a weaker sympathomimetic amine, its only FDA-approved use is for nasal congestion relief but has also found off-label use in the prevention of middle ear barotrauma during air travel for adults (12, 16).
Despite the long history of ephedra use, the sympathomimetic nature of ephedrine and pseudoephedrine can cause deleterious effects accidentally or when abused. These drugs can cause blurred vision, dizziness, nausea, and vomiting (10, 11). Of note, ephedra can cause adverse cardiovascular effects, such as palpitations, arrhythmia, and acute myocardial infarction (4). Chronic use has also been linked to hypertension, and one animal study suggests potential renal and salivary gland damage at high doses (17). These drugs are contraindicated with monoamine oxidase inhibitors , as this combination can cause an acute hypertensive episode (18). Several cases of sudden death have also been observed in those taking herbal supplements that contain ephedrine (19).
The Combat Methamphetamine Epidemic Act of 2005 established purchase limitations for products containing ephedrine and pseudoephedrine because both drugs are easily reduced to produce methamphetamine (Fig. 2). Although the intent of these limitations was to inhibit illicit methamphetamine production, pseudoephedrine can still be purchased behind the counter and has the potential for abuse itself. In case reports of abuse, massive dosages (3000–4500 mg of pseudoephedrine per day) were consumed for weight loss, euphoria, alertness, and improved mental acuity. Sudden cessation of the drug yielded restlessness, dysphoria, and has occasionally required hospitalization (20). Ephedrine alkaloids also have the potential for doping abuse in professional sports due to their effects on the respiratory and cardiovascular systems. Both drugs are included in the World Anti-Doping Agency list of prohibited substances. The detection limits in urine for ephedrine and pseudoephedrine are ≥10 µg/mL and ≥150 µg/mL, respectively (21).
Detection of ephedrine and pseudoephedrine is possible via FDA-approved amphetamine urine screening immunoassays as well as laboratory-developed gas chromatography-mass spectrometry and liquid chromatography-tandem mass spectrometry (LC-MS/MS) tests in both serum and urine. There is poor specificity for ephedra in the FDA-approved amphetamine immunoassays, as the target drug for these assays is d-methamphetamine. For example, the Roche Amphetamines II drug of abuse immunoassay exhibits an approximate cross-reactivity of 0.33% for (1R,2S)-ephedrine and (1S,2S)- pseudoephedrine (22). As such, the detection of ephedrine and pseudoephedrine via gas chromatography- mass spectrometry or liquid chromatography- tandem mass spectrometry is superior. However, because ephedrine and pseudoephedrine are structurally identical and only differ stereochemically (Fig. 2), their chromatographic separation can be challenging. Reversed-phase liquid chromatography-tandem mass spectrometry, hydrophilic interaction liquid chromatography, and gas chromatography-mass spectrometry performed with a chiral stationary phase (e.g., cyclodextrin) have all been successfully used to resolve the two drugs from one another (23–25).
Joshua Miller, PhD, is a second-year clinical chemistry fellow at the Mayo Clinic within the department of laboratory medicine and pathology, in Rochester, Minn.
The author has nothing to disclose.
Ephedra sinica, a species of ephedra (Ma huang), contains the alkaloids ephedrine and pseudoephedrine, which have been found to induce central nervous system stimulation, bronchodilation, and vasoconstriction with ephedrine toxicity associated with stroke, myocardial infarction and sudden death.
Ma huang has been used in traditional Chinese medicine for more than 5 millennia. Beverages made from the plant have been referred to under many names, e.g., yellow river, Mormon tea, and whorehouse tea. The jointed green stems of the ma huang are the chief photosynthetic organs of the plant and contain the alkaloids. In commercially available Ma huang products the percentage of ephedrine varies greatly from 1.1 to 15.3 mg per dosage unit. Ephedrine is well absorbed after oral administration is excreted primarily unchanged in the urine with a serum half-life of 2.7 to 3.6 hours. The pathogenesis of the cardiac toxic effects remains incompletely defined but probably related to increased blood pressure secondary to elevations in heart rate, cardiac output and peripheral resistance including vasoconstriction of the coronary arteries. Long term ephedrine use may lead to conditions seen with prolonged catecholamine excess resulting in fibrosis and even death.
On February 6th, 2004 the FDA issued a final rule prohibiting the sale of dietary supplements containing ephedrine alkaloids (ephedra) because such supplements present an unreasonable risk of illness or injury. The rule became effective 60 days after date of publication. On April 14, 2005 a Federal District Court in Utah struck down the FDA ban with the ruling only specific to Utah.
Overdoses of Ephedrine cause stimulation of the sympathetic nervous system with severe cases producing cardiac arrhythmia, increased blood pressure, and possible convulsions. Adverse reactions occur between one-half to two hours following ingestion of an excessive quality of the herb. Case reports describe multiple symptoms, including palpitations, nausea, tremulousness, abdominal pain, and vomiting. Patients present with abnormal electrocardiograms. Treatment of acute toxicity is based on controlling the stimulating effects of the drug. Treatment of acute agitation with benzodiazepines and neuroleptics has been used. A variety of medications have been used to lower the blood pressure and beta blockers are beneficial for tachyarrhythmias. Decontamination with activated charcoal has been used depending on the time of presentation.
The Toxin Spotlight is brought to you by ADLM's
